Tuesday, 4 December 2012

Thursday, 22 November 2012
HYPOTHYROIDISM
Thyroid Hormone Physiology:
● Thyroid hormones are necessary for the normal metabolism of human body● They have an important role to play in acceleration of growth and development
● They have a role in increasing body’s calorie production as per requirement
● Every tissue of body is affected directly or indirectly by the actions of the hormones
● The functions of thyroid hormones include:
● regulation of basal metabolic rate and adjustments of resting oxygen
consumption
● increased uptake, synthesis and utilization of glucose and heat production
● sympathomimetic effects including increased heart rate and force of contraction
Thyroid Hormone Control:
● Hypothalamic-pituitary-thyroid axis controls synthesis and release of thyroid hormones● The hypothalamus synthesizes a peptide thyrotropin releasing hormone (TRH)
● TRH stimulates pituitary thyrotrophs to produce thyroid stimulating hormone (TSH)
● TSH travels to and stimulates the thyroid gland, trophically to produce T4 and T3
T4 - T3 conversion:
● The major product of thyroid gland is T4. It accounts for 85% of thyroid hormone output
● T4 is metabolized by mono-deiodination to T3 , the more potent, biologically active form
● Circulating T4 has a half-life of seven days, whereas T3 has a half life of only one day
Thyroid Hormone Receptors:
● 3 receptors mediate the primary actions of thyroid hormone● These are named as TRa1, TRß1, and TRß2
● Interaction of T3 with its receptor promotes binding of cofactors
● These cofactors regulate expression of thyroid-hormone-responsive genes
● They act either through activation or repression of transcription
Hypothyroidism:
● Definition: It is the manifestation of effects of reduced thyroid hormones in humantissues
● 1.8% of total population affected and 2nd only to DM as commonest endocrine disorder
● Incidence increases with age and it is more common in females - 2-3% of older women
Classification of Hypothyroidism:
● Clinical Hypothyroidism (Overt Hypothyroidism)
● Symptoms are manifest - TSH is high and serumT3 and T4 are low
● Subclinical Hypothyroidism (Mild Hypothyroidism)
● No symptoms - Mild TSH
and Normal T3 & T4
● Euthyroid individual –
● Normal thyroid function Normal TSH – Normal T4 and T3
Etiology:
● PRIMARY HYPOTHYROIDISM - 99%● Hoshimoto’s thyroiditis is the most common cause
● Idiopathic hypothyroidism is also probably cases of old Hoshimoto’s Thyroiditis
● Irradiation or Surgical removal of thyroid or Drug therapy
● Iodine deficiency is still the most common cause of hypothyroidism
● Infiltrative Diseases: Sarcoidosis, Amyloidosis
● SECONDARY HYPOTHYROIDISM [1%]
● Decreased TSH production and resultant reduction in T4
● Pituitary neoplasm, Pituitary necrosis (Sheehan’s syndrome)
● Congenital hypopituitarism
● Hypothalmic dysfunction (Teritiary Hypothyroidism)
Hashimoto’s Thyroiditis:
● Dr. Hakaro Hashimoto was born in Iga-Ueno in Japan in the year 1881● He graduated in Medicine form Kyushu Imperial Medical University
● In 1912, he described the chronic thyroid disorder
● He termed it as Struma Lymphamatosa; but now called as Chronic Lymphocytic
Thyroiditis
● It is characterized by diffuse lymphocytic infiltration, fibrosis and parenchymal atrophy
Pathogenesis:
● Reduced metabolic rate causes reduced performance
● Hence weight gain occurs despite a poor appetite
● The pathology is deposition of Glycos-Amino Glycans(GAG) in tissues
● GAG is hygroscopic and causes mucinous edema
● Hence this results in a boggy non-pitting edema in tissues which are lax
● Skin and hair effects:
● Skin has reduced sweating and sebaceous secretions
● And there is thinning of epidermis, hyperkeratosis of stratum corneum
● Hence the skin is pale, cool, dry and coarse
● Capillary
fragility causes easy bruisability
● Scalp and body hair as well as the nails are dry and brittle
● Cardiovascular effects:
● Decrease in heart rate, pulse pressure and ¯ in the cardiac output
● ¯ blood supply and vasoconstriction of skin – results in cold intolerance
● Increased systemic vascular resistance – leads to increase in DBP
● Flabby myocardium and pericardial effusions are common
● ECG changes – sinus bradycardia, low voltage, ST & T changes
● Respiratory and GIT effects:
● Hoarseness of voice – due to GAG deposition in larynx
● Obstructive sleep apnoea to a thick tongue falling back
● Constipation due to reduced gut peristalsis
● Myxedema megacolon and Myxedema ileus are uncommon
● Neuromuscular effects:
● Slowed physical and mental functions leads to lethargy and increased somnolence
● Carpel tunnel syndrome due to deposition of GAG
● Delayed relaxation of ankle jerk is a useful bed side clinical finding
● Deafness and depression and rarely Myxedema madness may occur
Signs and Symptoms:
● These are non-specific and gradual in onset
● May be confused with other conditions like postpartum depression and Alzheimer’s
● One must maintain high index of suspicion
Common signs and symptoms:
Laboratory values
Additional Tests:
● Once diagnosis of primary hypothyroidism is made,● Additional imaging or serologic testing are unnecessary if gland is WNL
● In secondary cases, further testing with pituitary provocative testing
● imaging with CT scan annd or MRI to rule out microadenoma
● Evidence of ¯ of >1pituitary hormone indicates a panhypopituitary problem
● Serum cholesterol may be elevated. Complete lipid profile and ECG studies
● Prolactin levels are elevated in Secondary Hypopiuitarism
● Blood Haemoglobin and ferritin testing for anaemia are indicated in most cases
Antibodies in hypothyroidism:
● Anti Thyroid Per-Oxidase [anti microsomal] antibodies – Anti-TPO in most cases
● Anti thyroglobulin antibodies – Anti TG. Also found elevated in Hashimoto’s Thyroiditis
● Anti bodies against T3 and T4 in auto immune disease.
● Anti TSH Receptor and Anti-T3 T4 Receptor antibodies are also sometimes seen
● Anti gastric parietal cell antibodies are seen in 10% and this may lead to Pernicious
Anemia
Thyroid Hormone Replacement:
● Most healthy adults require 1.7 ugm/kg/day – 100-150ug/day● Levothyroxine cause increases in resting heart rate and BP
● Start at low doses in older and if cardiovascular compromise
● Elderly, dosage falls down to – 1.0 ugm/kg/day -50-100ug/day
● For full replacement children need up to 4ugm /kg/day
Monitoring thyroid function:
● Followed by serial TSH measurements● Changes in TSH levels lag behind serum T3 T4
● Resetting pituitary gland takes about 1 month
● So TSH not be checked sooner than 4 weeks
● Goal to keep TSH in lower half of normal range
● No need to monitor the T3 T4 levels normally
● In pituitary insufficiency T3 & T4 are followed
● Goal to keep T3 T4 in upper range of normal
● Once stable TSH or Free T4 monitored yearly
● Once stable it remains stable until 60-70 yrs
Pregnancy and Thyroid:
● During pregnancy the requirement for FT4 increases by 25-50%● Estrogens
® TBG
® ¯FT4 ® TSH
+ TPO
Ab ®Hypothyroidism
● Miscarriage, preterm delivery, preeclampsia & placental abruption● Can lead to ¯intellectual capacity & developmental delay in children
● (AACE) recommend universal thyroid testing for pregnant women
Myxedema coma:
● High mortality rate, despite intensive treatment
● Myxedema coma almost always occurs in the elderly
● Reduced consciousness, seizures + other features of hypothyroidism
● Precipitated by factors that impair respiration like sedatives
● Other precipitating factors - MI, CCF, CVA, UGIB and Pneumonia
● Myxedema coma-Treatment:
● Levothyroxine A single IV bolus of 500 g loading dose
● Levothyroxine is continued at a dose of 50 to 100 g/day
● If IV is not available the same initial dose by NG tube
● Supportive therapy:
● Correct metabolic disturbances & precipitating factors
● Hydrocortisone 50mg q6h should be administered
● Early use of broad-spectrum antibiotics for infection
● Space blankets should be used to prevent heat loss
● External warming for <300C, otherwise CV collapse
● Hypertonic saline if there is hyponatremia
● Hypotonic IV fluids avoided because water retention
● Intravenous glucose if there is hypoglycemia
● Sedatives avoided and blood levels monitored
● Ventilator support with regular blood gas analysis
Subclinical Hypothyroidism
● Definition: Biochemical evidence but no clinical evidence● No universal consensus in treatment of mildly elevated TSH
● Little risk if excessive treatment is avoided and clinical benefits
● Patients will progress to overt HYPO if TSH is >6mU/l
● Start with low dose 25-50 ug/day and slowly titrate upwards
Risk of over treatment
● Over treatment may result in atrial fibrillation● Otherwise there is a risk of development of osteoporosis
● Then there is a possibility of inducing frank hyperthyroidism
● Emotional lability, nervousness, irritability, poor concentration
● Start with low dose 25-50 ug/day and slowly titrate upwards
Friday, 16 November 2012
HEPATITIS B
LAMIVUDINE IN CHRONIC HEPATITIS B INFECTION |
| '48 weeks of treatment with lamivudine induces anti-HBe seroconversion in 27% of patients with HBeAg-positive chronic hepatitis, despite 38% developing HBV-DNA polymerase mutations. Treatment also improves histology and liver biochemistry.' |
| ADEFOVIR IN CHRONIC HEPATITIS B INFECTION |
| 'In HBeAg-positive chronic hepatitis treatment with 10 mg of adefovir for 48 weeks produces normal liver biochemistry in 48% (NNTB 3), suppresses serum HBV-DNA in 39% (NNTB 5) and leads to e antigen seroconversion in 14% (NNTB 16) of patients. In HBeAg-negative chronic hepatitis treatment with adefovir for 48 weeks reduces ALT to normal in 72% (NNTB 2.3) and renders serum HBV-DNA undetectable in 55% (NNTB 2) of patients.' |
| This is a nucleoside analogue which inhibits DNA polymerase and suppresses HBV-DNA levels. It is effective in improving liver function in patients with decompensated cirrhosis and may prevent the need for transplantation. Long-term therapy is complicated by the development of HBV-DNA polymerase mutants which may occur after 9 months of treatment and is characterised by a rise in viral load during treatment. These viral mutants are less hepatotoxic than native virus so the drug can often be continued (Box 23.40). Flares in transaminases occur when lamivudine is stopped if mutant virus is present, as native virus replaces mutant virus. |
| Adefovir |
| This is a nucleotide analogue that is phosphorylated to yield active drug which inhibits HBV-DNA polymerase. It reduces HBV-DNA levels by 3-4 logs, enhances the frequency of HBeAg seroconversion and leads to histological improvement, but is contraindicated in renal failure. The HBV-DNA mutants develop at a lower rate than with lamivudine, 2% being identified after 2 years of treatment (Box 23.41). Relapse occurs on stopping treatment and the optimum length of treatment remains unknown. Adefovir is effective in suppressing most of the lamivudine-induced DNA polymerase mutant viruses. |
| Other drugs |
| Other drugs which are currently been studied in chronic hepatitis B include tenofovir, which has anti-HIV efficacy, and L-deoxythymidine. The role of combination antiviral therapy, as used in HIV infection, is still unclear. |
| Liver transplantation |
| Historically, liver transplantation was contraindicated in the presence of hepatitis B because infection often recurred in the graft. However, the use of post-liver transplant prophylaxis with lamivudine and hepatitis B immunoglobulins has reduced the reinfection rate to 10% and increased 5-year survival to 80%, making transplantation an acceptable treatment option in selected cases. |
Prevention |
| AT-RISK GROUPS MERITING HEPATITIS B VACCINATION IN LOW ENDEMIC AREAS |
|
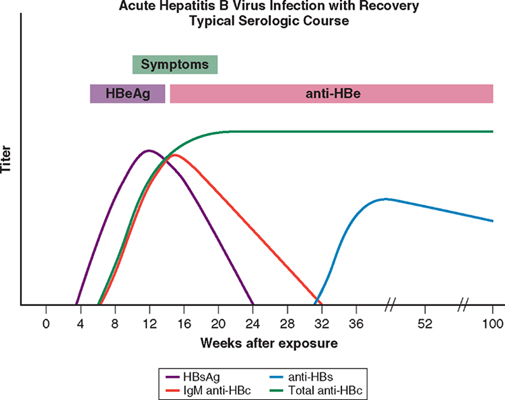
| Individuals are most infectious when markers of continuing viral replication, such as HBeAg, and high levels of HBV-DNA are present in the blood; they are least infectious when only anti-HBe is present with low levels of virus. HBV-DNA can be found in saliva, urine, semen and vaginal secretions. The virus is about ten times more infectious than hepatitis C, which in turn is about ten times more infectious than HIV. |
| A recombinant hepatitis B vaccine containing HBsAg is available (Engerix) and is capable of producing active immunisation in 95% of normal individuals. The vaccine gives a high degree of protection and should be offered to those at special risk of infection who are not already immune, as evidenced by anti-HBs in the blood . The vaccine is ineffective in those already infected by HBV. Infection can also be prevented or minimised by the intramuscular injection of hyperimmune serum globulin prepared from blood containing anti-HBs. This should be given within 24 hours, or at most a week, of exposure to infected blood in circumstances likely to cause infection (e.g. needlestick injury, contamination of cuts or mucous membranes). Vaccine can be given together with hyperimmune globulin (active-passive immunisation). |
| Neonates born to hepatitis B-infected mothers should be immunised at birth and given immunoglobulin. Hepatitis B serology should then be checked at 12 months of age. |
Prognosis |
Acute hepatitis |
| Full recovery occurs in 90-95% of adults following acute HBV infection. The remaining 5-10% develop a chronic infection which usually continues for life, although later recovery occasionally occurs. Infection passing from mother to child at birth leads to chronic infection in the child in 90% of cases and recovery is rare. Chronic infection is also common in immunodeficient individuals such as those with Down's syndrome or HIV infection. |
| Recovery from acute HBV infection occurs within 6 months and is characterised by the appearance of antibody to viral antigens. Persistence of HBeAg beyond this time indicates chronic infection. Combined HBV and HDV infection causes more aggressive disease. |
| Chronic infection |
| Most patients with chronic hepatitis B are asymptomatic and develop complications such as cirrhosis and hepatocellular carcinoma only after many years . Cirrhosis develops in 15-20% of patients with chronic HBV over 5-20 years. This proportion is higher in those who are e antigen-positive. |
Wednesday, 14 November 2012
HYPERTHYROIDISM
Hyperthyroidism
Disease processes associated with increased thyroid
secretion result in a predictable hypermetabolic state. Increased thyroid
secretion can be caused by primary alterations within the gland (Graves'
disease, toxic nodular goiter, toxic thyroid adenoma) or central nervous system
disorders and increased TSH-produced stimulation of the thyroid. Most
hyperthyroid states occur because of primary malfunction. Even more unusual
hyperthyroid states can result from mismanaged exogenous thyroid ingestion,
molar pregnancy with increased release of human chorionic gonadotropin, and
unusually, thyroid malignancy with overproduction of thyroid hormone.
Graves' Disease

Grave's disease is the most common cause of
hyperthyroidism (diffuse toxic goiter). This disease entity was originally
described by an Irish physician, Dr. Robert Graves, in 1835. Women between the
ages of 20 and 40 years are most commonly affected. The hyperthyroidism in
Grave's disease is caused by stimulatory autoantibodies to TSH-R. Although
several theories about the stimulus that initiates production of these
antibodies have been proposed, there is no universal agreement about the
etiology of the process. Genetic susceptibility to this disease is possible as
evidenced by the increased probability of Grave's disease in monozygotic twins.
Pathology
On microscopic examination, the follicles are small with
hyperplastic columnar epithelium. Hyperplasia of these cells is exhibited by
rapidly dividing nuclei and papillary projections of the follicular epithelium
within the central follicles. Increased deposition of lymphoid tissue is also
demonstrable in many patients with Graves' disease.
Clinical Features
A patient with classic Graves' disease usually has a
visibly enlarged neck mass consistent with a goiter that may demonstrate an audible bruit
secondary to increased vascular flow. Clinical thyrotoxicosis and exophthalmos
complete the classic triad of the disease. Hair loss, myxedema, gynecomastia,
and splenomegaly can accompany the clinical findings. Tracheal compression can
result in symptoms of airway obstruction, although acute compression with
respiratory distress is exceedingly rare.
The ocular consequences of prolonged and untreated
thyrotoxicosis, such as proptosis, supraorbital and infraorbital swelling, and
conjunctival swelling and edema, can be severe. The ophthalmopathy is thought
to be due to stimulation of the overexpressed TSH-R in the retro-orbital
tissues of Grave's patients. In its most severe form, spasm of the upper eyelid
resulting in retraction and visualization of a larger amount of sclera than
normal can lead to lid lag and exacerbation of the already swollen conjunctiva.
All these pressure-related phenomena can progress to decreased oculomuscular
movements, ophthalmoplegia, and diplopia. Optic nerve damage and blindness can
be a long-term consequence if the underlying condition is not corrected.
However, this is rarely seen currently with improved screening assays that
detect Grave's disease at early stages. Sustained hyperthyroidism is treated
aggressively to remove the stimulus to the retro-orbital tissues.
The hypermetabolic state of hyperthyroidism is clinically
manifested as sweating, weight loss, heat intolerance, and thirst.
Cardiovascular stress can be demonstrated by high-output cardiac failure,
congestive heart failure with peripheral edema, and arrhythmias such as
ventricular tachycardia or atrial fibrillation. Gastrointestinal signs may
include diarrhea and electrolyte wasting. The menstrual cycle can be altered to
the point of amenorrhea. Psychiatric signs may include altered sleep patterns,
emotional mood swings, fatigue, excitability, and agitation.
Diagnosis

An enlarged smooth thyroid mass and signs and symptoms of
thyrotoxicosis suggest the diagnosis. A cost-effective workup can include an
extensive history, physical examination, and thyroid function tests. In
addition to elevated levels of T3 and T4, a decreased or
undetectable level of TSH is demonstrated. Thyroid antibodies are usually detected
in elevated quantities. An 123I
radionuclide scan demonstrates diffuse uptake throughout an enlarged gland.
Ultrasound or computed tomography (CT) of the neck can be used to evaluate clinical
landmarks . However, the absolute requirement of CT and ultrasound for
preoperative assessment is not universally agreed on.
When a diagnosis of Graves' disease has been made,
therapy is initiated rapidly to ameliorate symptoms and decrease thyroid
hormone synthesis. This is particularly crucial for patients with
vision-threatening exophthalmos. The former is accomplished with β-blocker
therapy, which is started immediately, and the latter with thionamide,
radioactive iodine ablation, or surgery, each of which is equally effective in
normalizing serum thyroid hormone levels within 6 weeks. Clearly, patients with
Grave's disease need to be educated regarding appropriate choices, the risks
associated with each treatment, and the expectation of complete success.
Radionuclide Therapy
Radioiodide ablation with 131I
is the therapy of choice in the United States. It ablates the thyroid within 6
to 18 weeks. Patients with mild, well-tolerated hyperthyroidism can safely
proceed to radioactive iodine ablation immediately. However, those who are
elderly or severely thyrotoxic may require pretreatment with a thionamide. The
overall cure rate with radioactive iodine is 90%. Hypothyroidism will develop
in cured individuals, hence the need for careful measurement of thyroid hormone
and TSH levels at regular intervals after therapy. Most patients are candidates
for radioactive iodine; exceptions include women who are pregnant or lactating
or those with a suspicious nodule.
Advantages of 131I
therapy include avoidance of surgery and the associated risks of recurrent
laryngeal nerve damage, hypothyroidism, or postsurgical recurrence. It may be
that 131I therapy is more
cost-effective in the long run; however, the financial advantage is not as
clear if repeated 131I therapy is
needed. Additional disadvantages include exacerbation of cardiac arrhythmias,
particularly in elderly patients, possible fetal damage in pregnant women,
worsening ophthalmic problems, and rare, but possibly life-threatening thyroid
storm.
Antithyroid Medication
PTU and methimazole inhibit the organification of
intrathyroid iodine, as well as the coupling of iodotyrosine molecules to form
T3 and T4. PTU has the additive effect of blocking peripheral
conversion of T4 to T3. This is important because
peripheral access to T3 and T4 has multiple hyperdynamic
and hypermetabolic effects. Additionally, the peripheral adrenergic effects of
thyrotoxicosis can be modulated by the use of β-blocking agents such as
propranolol. Corticosteroids in combination with β-blockers can help gain rapid
control of the hypermetabolic effects of increased peripheral T4 and
T3. Patients may choose a trial of antithyroid medication over
radioactive iodine therapy. The goal of this therapy is to attain euthyroidism;
however, hypothyroidism may result and necessitate thyroid hormone replacement.
Antithyroid medication is effective in gaining rapid control of thyrotoxicosis,
but the relapse rate after discontinuation of medication may approach 50% 12 to
18 months after cessation. Additionally, patients need to be monitored for side
effects of the drugs, which may include granulocytopenia and, in rare
instances, aplastic anemia. Other side effects include fever, polyarteritis, and
rash.
Thyroid Resection
Surgery is advocated by a minority of thyroid specialists
in the United States. It is primarily indicated for patients who have an
obstructive goiter, have a fear of radioactivity, are noncompliant, or have had
an adverse effect with thionamide drugs. Additional candidates are pregnant
patients or those with a suspicious nodule. Advantages of surgical ablation of
the thyroid include rapid, effective treatment of thyrotoxicosis without the
necessity for medications and their accompanying side effects. The amount of
residual tissue is a subject of debate. Complete ablation of thyroid tissue
requires total thyroidectomy, which is associated with the highest rates of
hypoparathyroidism and recurrent laryngeal nerve damage. Some groups have
reported that total thyroidectomy is the most effective way to treat patients
with severe Graves' disease because it offers the lowest rate of relapse. It
may be that patients, particularly those with ophthalmopathy, are stabilized
most successfully by total thyroidectomy. Removal of the entire antigenic focus
may be the most likely explanation for this observation. Other subtotal
resections include near-total thyroidectomy or subtotal thyroidectomy.
Careful documentation of euthyroid status before surgery
in all hyperthyroid patients is mandatory. If the patient is not properly
treated preoperatively, thyroid storm can be life threatening. Fortunately,
this complication is rarely encountered if appropriately anticipated. Thyroid
storm is manifested by severe tachycardia, fever, confusion, vomiting to the
point of dehydration, and adrenergic overstimulation to the point of mania and
coma after thyroid resection in an uncontrolled hyperthyroid patient. The best
way to treat thyroid storm is preoperative anticipation and preparation.
Additionally, all patients undergoing general anesthesia are checked for
undiagnosed hyperthyroidism, if clinically suspected. Treatment of a patient
with overt thyroid storm includes rapid fluid replacement and institution of
antithyroid drugs, β-blockers, iodine solutions, and steroids. In
life-threatening circumstances, peritoneal dialysis or hemodialysis may be
effective in lowering T4 and T3 levels.
Toxic Nodular Goiter/Toxic
Adenoma
Toxic nodular goiter, also known as Plummer's disease,
refers to a nodule contained within an otherwise goitrous thyroid gland that
has autonomous function. It usually occurs in the setting of a patient with
endemic goiter. Increased thyroid hormone production occurs independent of TSH
control. Such patients generally have a milder course and are older than those
with Graves' disease. The thyroid in these patients may be diffusely enlarged
or associated with retrosternal goiters. Initial symptoms are mild, peripheral
thyroid hormone levels are elevated, and TSH levels are suppressed. Antithyroid
antibody levels are usually decreased. The diagnosis is generally confirmed
after clinical suspicion, and an 131I
radionuclide scan is performed that localizes one or two autonomous areas of
function while the rest of the gland is suppressed ( Fig. 36-6 ). Toxic nodular
goiter can be treated with thionamides, radioiodine therapy, or surgery;
however, the latter two are preferred because these nodules rarely resolve with
prolonged thionamide therapy. Radioiodine is widely used for patients with
toxic adenomas, although it is not as effective as in Grave's disease. Most
patients are euthyroid after radioiodine therapy because the radioiodine preferentially accumulates
in hyperfunctioning nodules. The surgical approach is lobectomy or near-total
thyroidectomy, particularly when clinical symptoms are pronounced. In the case
of a single, hyperfunctioning adenoma, lobectomy is generally curative.
Nontoxic Goiter
Multinodular Goiter
Multinodular goiter describes an enlarged, diffusely
heterogeneous thyroid gland. Initial findings may include diffuse enlargement,
but asymmetric nodularity of the mass often develops. The cause of this mass is
usually iodine deficiency. Initially the mass is euthyroid, but with increasing
size, elevations in T3 and T4 can occur and gradually
progress to clinical hyperthyroidism. Workup and diagnosis involve evaluation
of thyroid function tests. Ultrasound and radioisotopic scanning demonstrate
heterogeneous thyroid substance. Nodules with poor uptake can appear as lesions
suggestive of malignancy. The incidence of carcinoma in multinodular goiter has
been reported to be 5% to 10%. Therefore, FNA for diagnosis and resection for
suspicious lesions is considered.
Substernal Goiter
A substernal goiter is an unusual manifestation of
intrathoracic extension of an enlarged thyroid that generally occurs as a
result of multinodular goiter. Most intrathoracic or substernal goiters are
labeled secondary because they are enlargements or extensions of
multinodular goiters based on the inferior thyroid vasculature. They expand
downward into the anterior mediastinum. The extremely rare (∼1%) primary substernal goiter arises as
aberrant thyroid tissue within the anterior or posterior mediastinum and is
based on the intrathoracic vasculature and not supplied by the inferior thyroid
artery.
Special Considerations for Patients With Goiter
Patients with an enlarged thyroid mass (>5 cm) can
have a spectrum of symptoms ranging from none to severe dysphagia, choking, and
pain. Occasionally, the diagnosis is suggested by the presence of an anterior
mediastinal mass on chest radiography. In 10% to 20% of cases, an asymptomatic
patient may have no palpable abnormality in the cervical area and a completely
intrathoracic lesion.
CT is the preferred imaging study, and all regions from
the mandible to the upper part of the abdomen are included in the scan. The
lesion itself is scrutinized. Benign goiters have rounded, smooth borders.
Thyroid malignancies generally have more ill-defined borders. CT also allows
evaluation of regional lymph nodes and metastasis. If the patient has a history
of cervical pain and night sweats, a diagnosis of lymphoma is considered. The
use of FNA with CT guidance is important to secure a tissue diagnosis. Magnetic
resonance imaging (MRI) does not usually add significant information to a
well-performed CT scan. For patients with an intrathoracic lesion and a history
of coughing, preoperative bronchoscopy can give important information about
vocal cord status and possible luminal invasion by a malignancy.
Almost all
goiters and other thyroid masses are initially approached surgically through a
cervical incision. Goiters are usually mobilized easily, even when they are
substernal. The blood supply is generally based on the inferior thyroid artery,
which is in its normal position and allows even large substernal masses to be
gently mobilized into the neck. Careful attention must be directed to the
location of the esophagus, trachea, and recurrent laryngeal nerve. The
esophagus can be injured by overaggressive manipulation of the thyroid mass.
The recurrent laryngeal nerve is usually displaced posteriorly and inferiorly;
however, it can be draped anteriorly over the mass and damaged in that
position. Great care must be exercised in mobilization of the mass until the
nerve is identified. The cervical incision is extended to a median sternotomy
if there is significant bleeding from the anterior mediastinum, if the anatomy
and location of the recurrent laryngeal nerve are in doubt, or if the mass
cannot be mobilized through the surgical field.
Tuesday, 13 November 2012
MYXOEDEMA
 Myxoedema means severe hypothyroidism in adults and signs
and symptoms are accentuated. The facial appearance is typical
Myxoedema means severe hypothyroidism in adults and signs
and symptoms are accentuated. The facial appearance is typical
There is often supraclavicular puffiness, a malar flush and
a yellow tinge to the skin
Myxoedema coma, characterised by altered mental status,
hypothermia and a precipitating medical condition, for example cardiac failure
or infection, carries a high mortality rate
Treatment
Thyroid replacement: Either a bolus of 500 mg T4 or 10 micro
gram T3 either intravenously or orally every 4-6 hours
For hypothermia(<30 degree) body is warmed slowly
Intravenous broad spectrum antibiotics and steroids
Primary or atrophic myxoedema is considered to be an
autoimmune disease similar to chronic lymphocytic thyroiditis Hashimotos) but
without Goiter formation,and there is delay in diagnosis and hypothyroidism is
severe
Ref : Bailey and Love
RETRO-STERNAL GOITRE
Very few retrosternal goitre arise from ectopic thyroid
tissue, most arise from lower pole of nodular goitre. If neck is short and
pretracheal muscles are strong especially in men the negative intrathoracic
pressure tends to draw these nodules into superior mediastinum
Clinical Features
 ·
Dyspnoea, particularly at night,cough, stridor
·
Dyspnoea, particularly at night,cough, stridor
·
Dysphagia
·
Engorgement of facial, neck,superficial chest
wall veins: occurs in cases of obstruction of superior venacava
·
Recurrent nerve paralysis; the goiter may be
also malignant or toxic
Diagnosis
·
Chest and thoracic inlet Radio graphs
·
CT scan, MRI
·
Flow-volume pulmonary function test; to detect
degree of obstruction
Treatment
No role for anti-thyroid drugs and radio-iodine,resection is
carried out from neck sometimes median sternotomy is needed. Fragmentation during resection must be avoided in case of malignancy. Recurrent laryngeal N
injury is common.
Ref: BAILEY AND LOVE
Friday, 9 November 2012
HEPATITIS D (DELTA VIRUS)
The HEPATITIS D virus (HDV) is an RNA defective virus which
has no independent existence,it requires HBV virus for replication and has got
same mode of transmission.It can infect those with HBV and can also cause
superinfection on chronic carriers for HBV
Infection is self limiting along with HBV. Simultaneous
infection with HBV and HCV Leads on to rapid progressive Hepatitis leading on
to cirrhosis
Mode of transmission is similar to HBV
Investigations
HDV virus contain a single antigen to which body makes
anti-HDV antibody, delta antigen appears in blood transiently, diagnosis depends
on anti-HDV. Antibody usually disappears after 2 months
Super infection produce high titres of anti-HDV.
Management
Effective management of hepatitis B effectively prevents
hepatitis D
Subscribe to:
Comments (Atom)